
Understanding the Affordable Care Act, Part 3: Who Pays for the ACA?

ACA Funding in Context: Why the Numbers Matter
Before diving into how the Affordable Care Act is funded, it helps to step back and look at the broader fiscal picture. Federal healthcare spending is now one of the largest components of the U.S. budget, competing with Social Security, defense, and interest on the debt for limited public dollars. That reality shapes every ACA funding debate. The law’s subsidies may represent only one part of total healthcare spending, but they sit inside a much larger and more expensive system—one in which even relatively modest policy changes can affect federal deficits, insurance affordability, and coverage for millions of Americans.
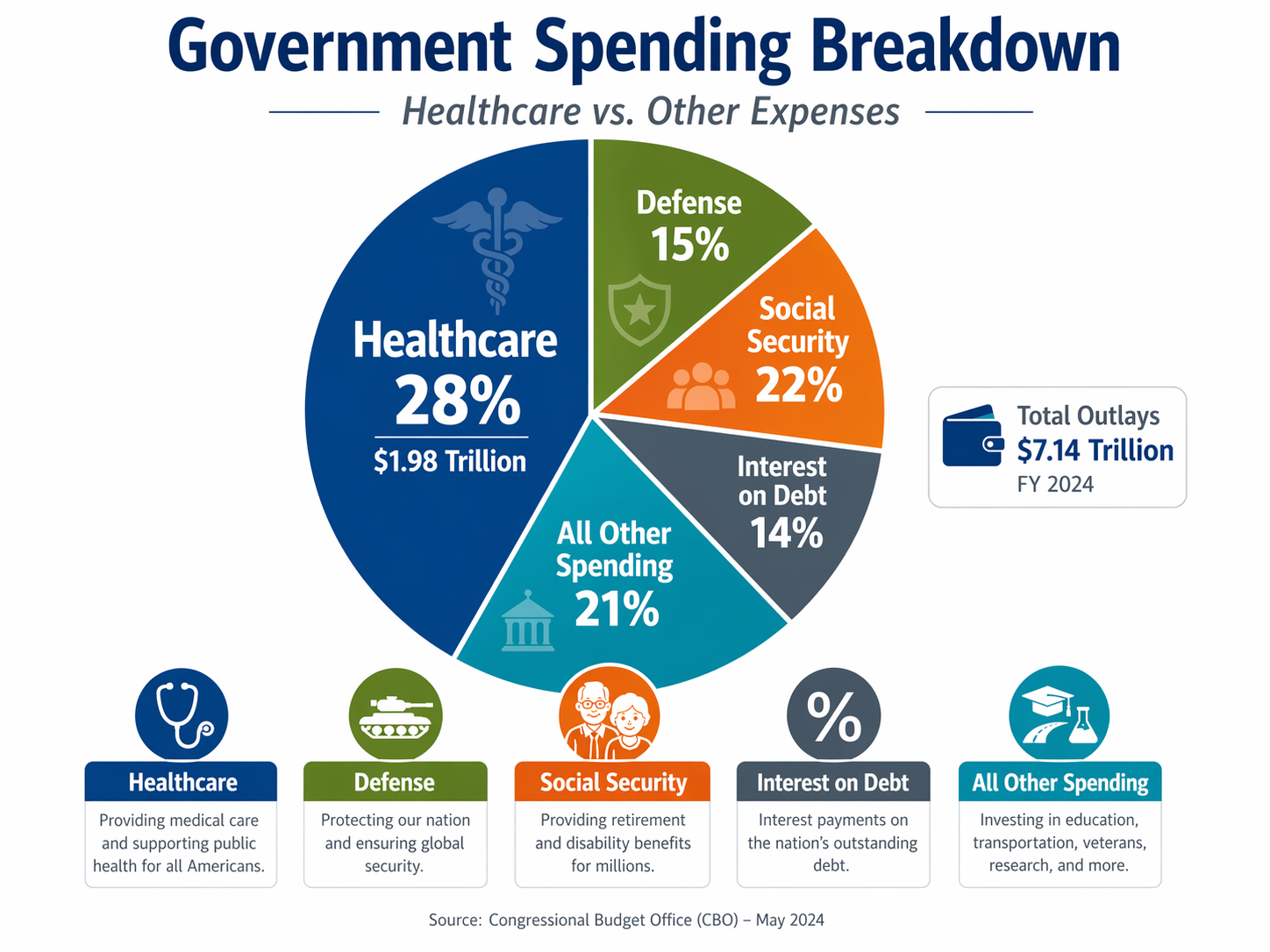
The overall government budget in this pie chart shows just how large healthcare has become within the federal fiscal picture. In FY2025, total federal outlays were about $7.01 trillion, and Health plus Medicare accounted for roughly $1.98 trillion, or about 28% of all federal spending. That puts healthcare in the same tier as the government’s other biggest obligations, including Social Security, net interest on the debt, and national defense. The challenge is straightforward but profound: when one category consumes more than a quarter of total federal spending, even modest cost growth can place enormous pressure on taxpayers, deficits, and the government’s ability to fund other priorities.
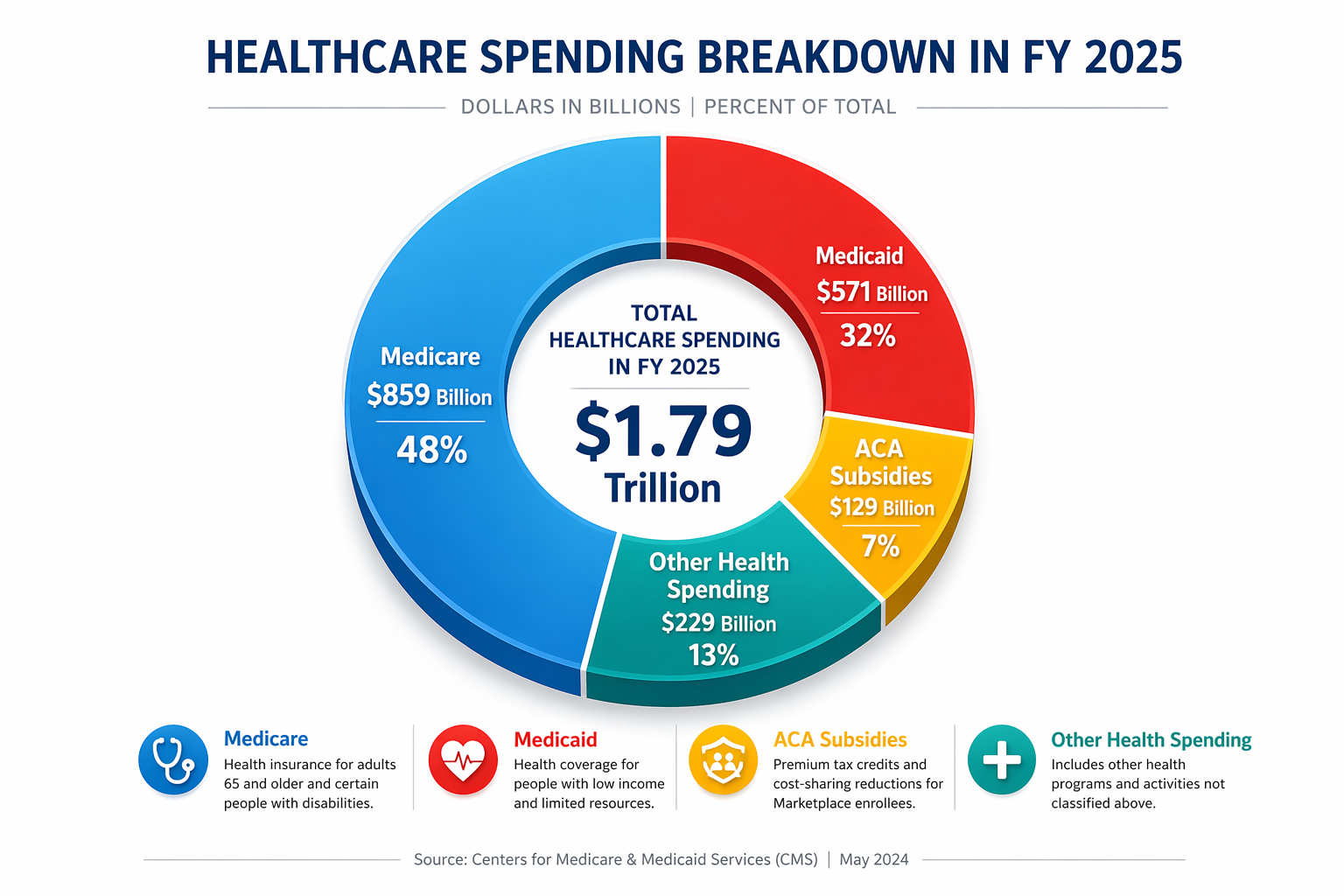
This pie chart breaks that large commitment into more understandable parts. Medicare is the largest share, reflecting the cost of caring for an aging population; Medicaid is the next major component, supporting low-income Americans, children, many disabled individuals, and much of the nation’s long-term care; ACA subsidies are smaller but still important; and the remaining category includes other federal health programs. The challenge is that each piece of this spending pie supports a different vulnerable population, so reducing costs is rarely simple. In practice, efforts to cut healthcare spending often entail difficult trade-offs among benefits, access, provider payments, and premiums.
How COVID-Enhanced Subsidies Affected the Budget
The COVID-era expansion of ACA subsidies mostly added to federal deficits rather than directly cutting other major budget items. The enhanced premium tax credits created in 2021 made coverage more affordable and expanded eligibility, but the budget effect was straightforward: the federal government spent more on subsidies and financed those added costs largely through borrowing, not by visibly reducing defense, education, or other major programs. Treasury notes that federal deficits are primarily financed through borrowing from the public, which means new health spending often shows up first as added debt rather than as an immediate cut elsewhere.
The later extension of those subsidies through the Inflation Reduction Act was different because it was paired with offsetting savings, especially from prescription-drug reforms. CBO found that the IRA’s drug-pricing provisions would reduce deficits by about $237 billion over 2022–2031, helping counterbalance the cost of maintaining broader subsidy support. That is the central challenge: expanding healthcare subsidies can improve affordability and coverage, but unless lawmakers pair them with savings or new revenue, they add to debt and intensify pressure on the rest of the budget over time.
ACA Funding Sources
Public debates about healthcare policy often focus on what programs do, but much less attention is paid to how they are actually funded. The Affordable Care Act (ACA), like many major federal programs, relies heavily on general federal revenues—the large pool of tax dollars collected from individuals and businesses. Understanding how those dollars move through Congress and the federal government helps clarify where spending decisions are made, which programs receive automatic funding, and how taxpayer dollars ultimately support federal programs.
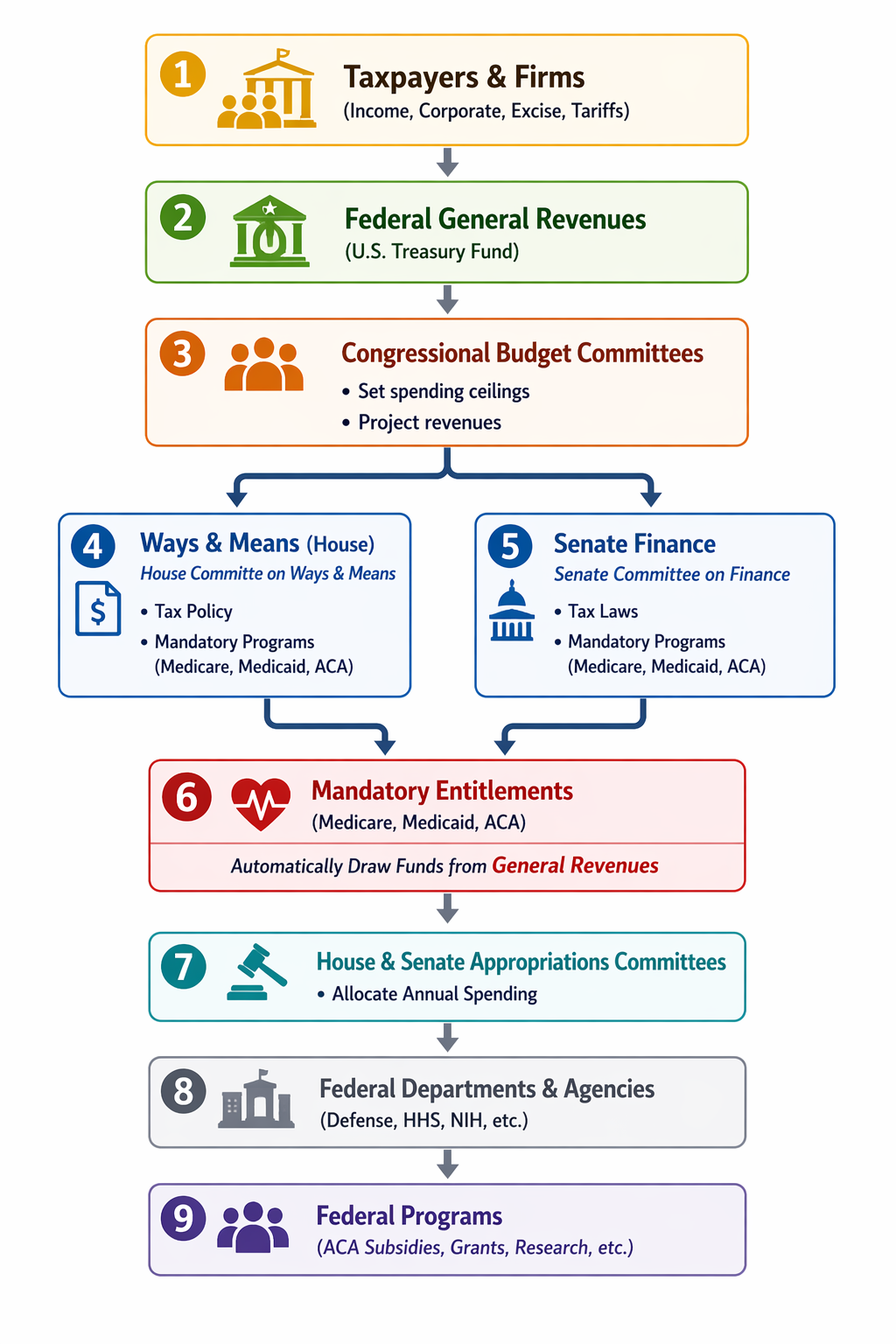
This flowchart shows how money collected from taxpayers and businesses flows through the federal government before being spent on programs such as Medicare, Medicaid, and Affordable Care Act (ACA) subsidies. Taxes on income, corporations, and certain goods first go into the U.S. Treasury’s general revenue pool, which functions as the government’s main operating fund. From there, Congress sets the overall fiscal framework through its Budget Committees, which estimate revenues and establish spending targets. Key committees—particularly the House Ways and Means Committee and the Senate Finance Committee—write the laws that govern taxes and mandatory programs such as Medicare, Medicaid, and ACA subsidies. Because these programs are considered mandatory entitlements, the spending occurs automatically once the law defines who qualifies and how much they receive.
A second part of the system handles discretionary spending, which must be approved each year by Congress. This is the responsibility of the House and Senate Appropriations Committees and their twelve subcommittees, which allocate funding for government departments and agencies such as the Department of Defense, the Department of Health and Human Services, the National Institutes of Health, and many others. Those agencies then carry out federal programs ranging from research grants to healthcare programs to national defense. In short, some spending—especially entitlement programs—flows automatically based on existing law, while other spending must be approved annually through the appropriations process.
This funding structure has advantages but also carries some long-term risks. Since the program relies on general revenues rather than a dedicated funding source, its costs compete with many other federal priorities such as defense, education, and infrastructure. As healthcare spending rises over time, the amount required to support ACA subsidies can also grow. When that happens, policymakers face difficult choices: increase taxes, borrow more money, or reduce spending in other areas. In a large federal budget, these trade-offs can become significant, particularly if multiple entitlement programs expand simultaneously.
Another risk is that programs funded from general revenues can become less transparent to the public. Because the funding comes from a broad tax base rather than a specific tax tied to the program, it can be harder for voters to see the direct connection between the benefits provided and the costs required to sustain them. Over time, if program costs grow faster than expected, the burden shifts to future taxpayers through higher taxes or increased federal debt. For this reason, debates about the ACA—and about entitlement programs more broadly—often focus not only on their benefits but also on how to ensure they remain financially sustainable for the long term.
IRS Tax Provisions. The IRS phrase “ACA tax provisions” should not be misunderstood as a dedicated funding stream for the entire law. These provisions include tax credits, reporting rules, employer requirements, and targeted taxes such as the Additional Medicare Tax and Net Investment Income Tax. They help support and administer the ACA, but they offset only part of the cost of Marketplace subsidies and Medicaid expansion; the rest flows through the broader federal budget.
References
U.S. Treasury Fiscal Data. America’s Finance Guide: Federal Spending.
Accessed March 17, 2026.
https://fiscaldata.treasury.gov/americas-finance-guide/federal-spending/Congressional Budget Office. The Budget and Economic Outlook: 2026 to 2036.
February 11, 2026.
https://www.cbo.gov/publication/62105Congressional Budget Office. Estimated Budgetary Effects of Subtitle I of Reconciliation Recommendations of the House Committee on Ways and Means.
February 18, 2021.
https://www.cbo.gov/system/files/2021-02/hwaysandmeansreconciliation.pdfCongressional Budget Office. How CBO Estimated the Budgetary Impact of Key Prescription Drug Provisions in the 2022 Reconciliation Act.
February 17, 2023.
https://www.cbo.gov/publication/58850KFF. Enrollment Growth in the ACA Marketplaces.
April 2, 2025.
https://www.kff.org/affordable-care-act/enrollment-growth-in-the-aca-marketplaces/
Looking Ahead
In the next post, we will turn from policy to practice by examining real-world patient examples that show how the ACA shapes coverage, out-of-pocket costs, access to care, and financial stability.