
Briefs: What the Measles Resurgence Really Shows
A physician’s evidence-based look at outbreaks, vaccination, and public trust.
I wrote this because I am a physician, and I have spent much of my professional life trying to separate the signal from the noise. On questions like measles, that discipline matters. The subject is emotionally charged, politically distorted, and easy to reduce to whatever conclusion one already prefers. But measles is still, fundamentally, a medical and public-health problem. The correct starting point is not outrage. It is evidence.
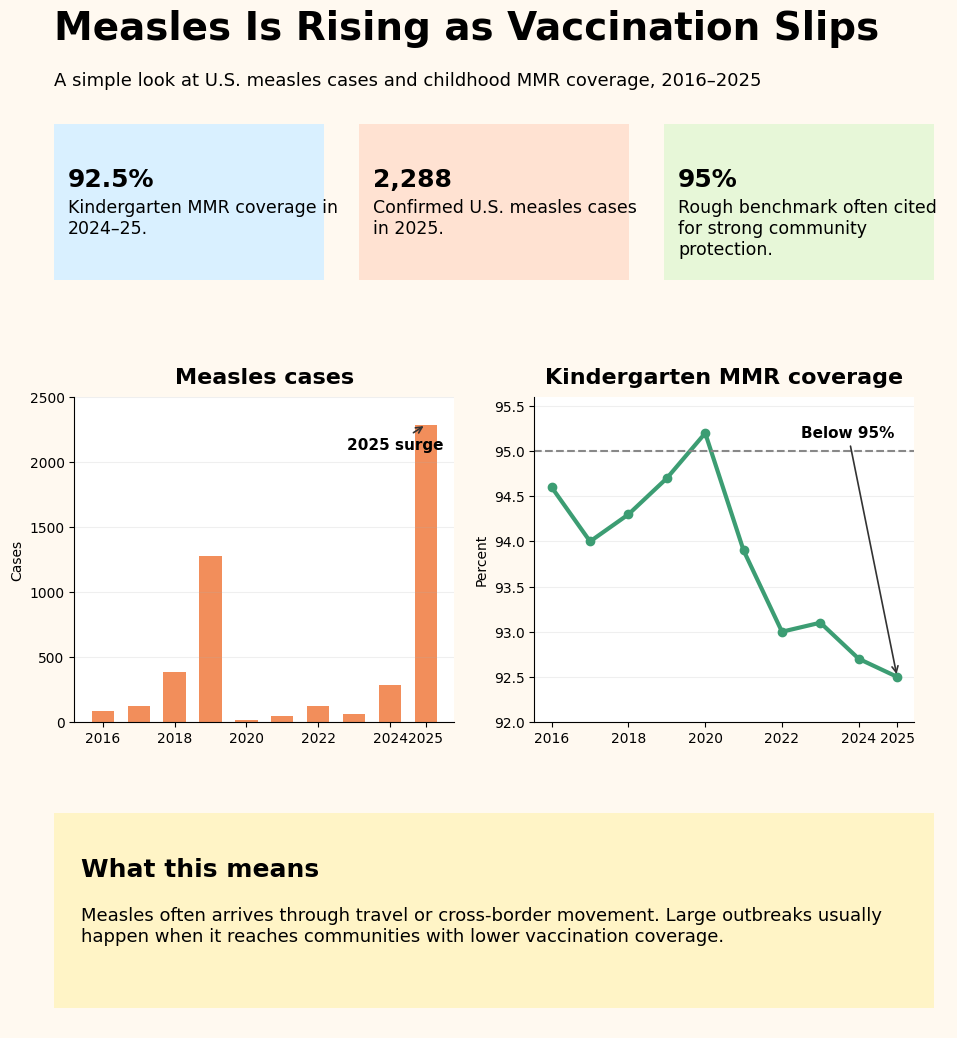
The evidence points to a pattern that is neither mysterious nor especially flattering to any side in the debate. In 2025, the United States recorded 2,288 confirmed measles cases, with 48 outbreaks, and 90% of those cases were outbreak-associated. At the same time, national kindergarten vaccination coverage for measles, mumps, and rubella fell to 92.5%in the 2024–25 school year, down from 95.2% in 2019–20. CDC also reported that about 286,000 kindergartners were attending school without documentation of a completed MMR series in 2024–25. That does not guarantee an outbreak every year, but it does create a more fragile system.
That fragility helps explain why measles has returned in spikes rather than as a smooth, predictable increase. The US saw a major outbreak year in 2019, quieter years around the pandemic, and then a large resurgence in 2025. The CDC’s description of the mechanism is informative: larger U.S. outbreaks typically follow movement of an infected individual into close-knit communities with low vaccination coverage. That means measles often enters through travel, but it becomes a serious outbreak only when it reaches a cluster of susceptible individuals. Through April 17, 2025, the CDC reported 800 cases, 82% of which were tied to a single outbreak in New Mexico, Oklahoma, and Texas.
That is why I do not find the simplest political explanations very satisfying. It is too easy to say this is all Robert F. Kennedy Jr.’s doing. It is not. The erosion in vaccination coverage predates his tenure. The system was already weakening before he arrived. But it is also too easy to say national rhetoric does not matter. It does. When vaccine confidence is already fraying, vague or inconsistent leadership can make a bad situation worse. The deeper point, though, is that the vulnerability was already there: lower vaccination rates, more exemptions, and more communities in which herd immunity had thinned.
It is also incorrect to blame local pediatricians. The KFF/Washington Post survey found that parents still trust their child’s pediatrician more than any other source for vaccine information. The problem is that physicians are now competing with a much broader culture of doubt. Parents who delay or skip vaccines generally do not cite cost or access as the main reason. They are citing safety concerns, side effects, and skepticism about whether all vaccines are necessary. In other words, this looks less like a collapse of medical access and more like a collapse of confidence.
The immigration question also deserves a thoughtful analysis. Because Texas and New Mexico are border states, some have raised the question as to whether immigration played a role. The fair answer is yes, cross-border movement can matter. Measles does not respect state lines or national borders. Travel, migration, and family networks can all move the virus from one place to another. But that is not the same thing as saying undocumented immigrants caused the West Texas outbreak. Publicly, Texas officials stated that they did not know how that outbreak began. There is no public evidence indicating that an undocumented immigrant is the index case.
CDC’s own early-2025 data also argue against making immigration the main story. Of the 48 internationally imported measles cases reported through April 17, 44 were U.S. residents, not foreign arrivals. That is an important observation. A border state can certainly be exposed to regional migration, but the available evidence does not support a broad claim that illegal immigration was the source of the outbreak. The more defensible conclusion is narrower: measles can move across borders, but once it arrives, local vaccination coverage determines whether it fizzles or spreads.
Perhaps the border may help explain how sparks move around. It does not explain why the fire catches. A community with strong vaccination coverage is far less likely to sustain a large outbreak. A community with lower coverage is far more likely to do so. That is not ideology. It is simply the epidemiologic pattern described by the CDC.
As a physician, I find that conclusion both sobering and clarifying. Sobering, because it means this problem is not likely to yield to one speech, one headline, or one political villain. Clarifying, because it tells us where to look if we are serious about prevention: school-entry policies, exemption policies, local vaccine administration, and public trust. We can have political arguments about Kennedy, about the border, and about the failures of modern public health. Some of those arguments are worth having. But the evidence keeps bringing us back to the same place. Measles returns when the virus enters a population with lower immunity.
Closing Thoughts
As a physician, I find less value in forcing a complicated public-health problem into a single political frame. Measles is not returning because of one person, one party, or one argument. It is returning because a highly contagious virus has found more opportunities to spread within the herd. That is supported by the data, and it is the one we should be most careful not to lose sight of amid the noise.
I wrote this because I value evidence, but also because experience teaches humility. Public-health failures are rarely monocausal. They usually reflect a chain of smaller failures: declining trust, uneven policy, inconsistent messaging, and communities that have become more vulnerable than many people realize. Measles is reminding us that the consequences of that erosion are not theoretical.
If there is a lesson here, it is not simply that measles has come back. It is that protection can weaken quietly, and that by the time the problem becomes visible, the underlying conditions have often been in place for years. That is why the most useful response is not reflexive blame. It is a renewed commitment to clear evidence, sound policy, and the kind of public trust that preventive medicine depends on.
References
CDC, Measles Cases and Outbreaks
CDC, Vaccination Coverage and Exemptions among Kindergartners, 2024–2025
CDC MMWR, Measles Update — United States, January 1–April 17, 2025
KFF / Washington Post, Survey of Parents
Texas Tribune, Texas officials still don’t know how West Texas measles outbreak started